Lung Cancer | Pancoast
Published on Feb 16, 2021
71 male
First appointment
- 3 Month history of Right rhomboid pain.
- Aggravated by shoulder movements.
- Struggles to get to sleep and occasionally wakes up.
- No P+N or numbness. No dizziness, diplopia, dysarthria, dysphagia, drop attacks, nausea.
Exam
- Slight winging right scapula.
- Full shoulder ROM
- Full shoulder strength
Provisional Diagnosis
Subacromial Impingement
1st Review – 1 month later
- 4 month history right scapular medial border pain.
- Reports pain to be worse. Had to call paramedics who prescribed codeine. No help.
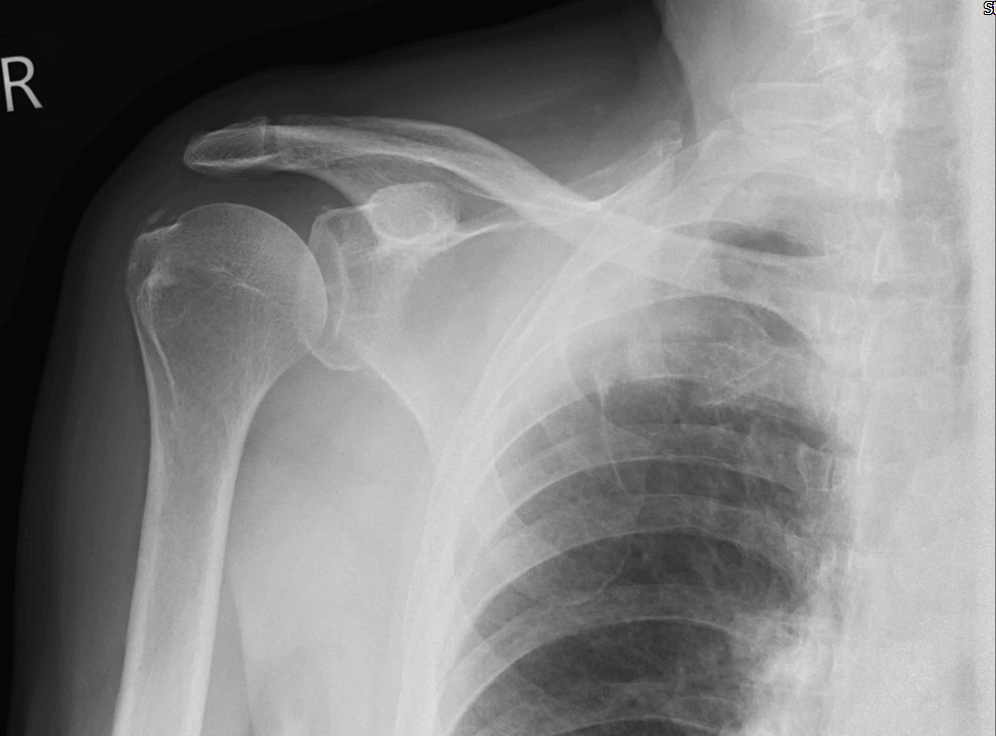
- GP arranged blood tests and Shoulder X-ray.
Investigations
- ESR: 24
- CRP: 23
- X-ray shoulder – Mild supraspinatus calcification reported.
Started on Amitriptyline by GP. Continues to take 8 paracetamol per day.
Review – contd
Reports waking up 2-3 times per night
- Feeling well
- No weight loss
- No temperature
- No night sweats
- Able to lie supine comfortably.
- Unable to do exercises as too painful.
- Tender T 5/6 level, causes radiation of pain to right medial scapular region.
- Active thoracic ROM limited due to pain.
- No myotomal weakness – upper limbs
- Deep tendon jerks – bilaterally brisk – upper and lower limbs.
- Hoffman -ve
- No gait disturbances.
Assessment
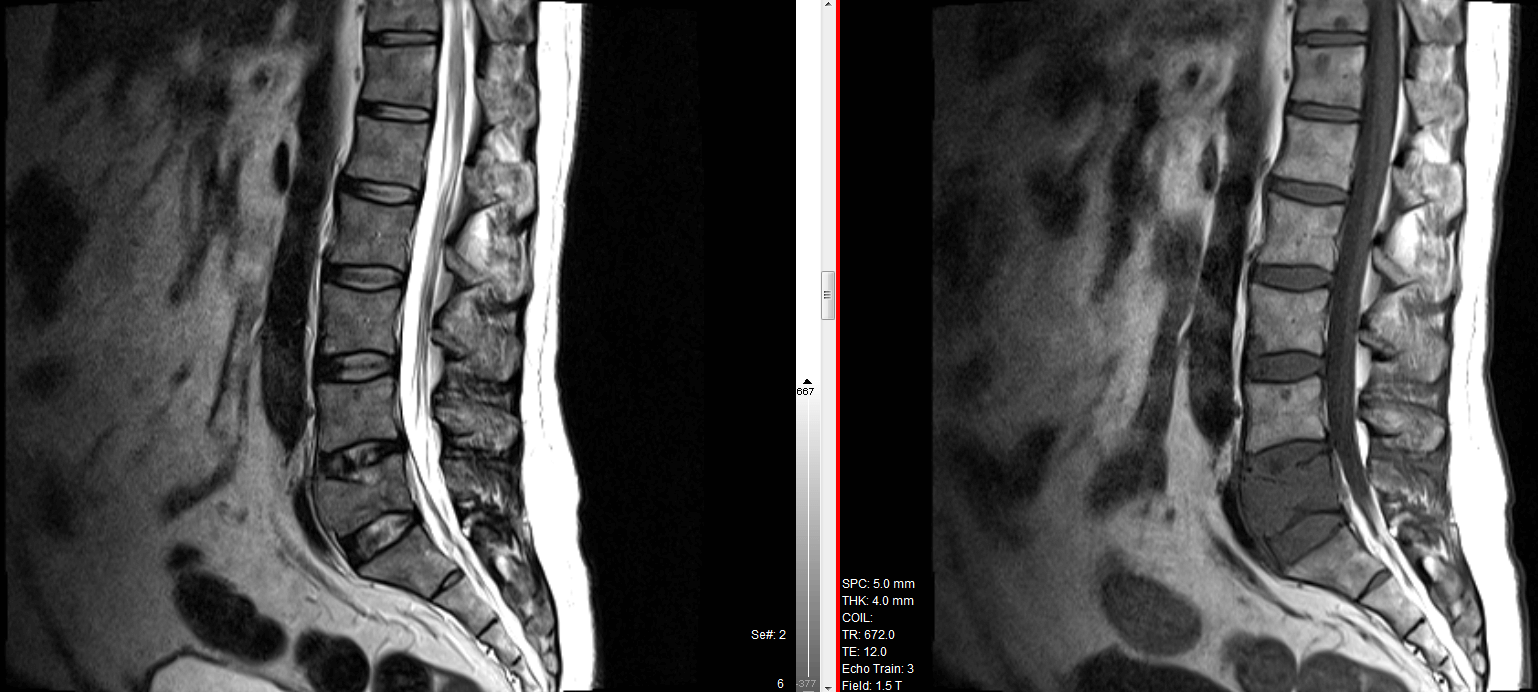
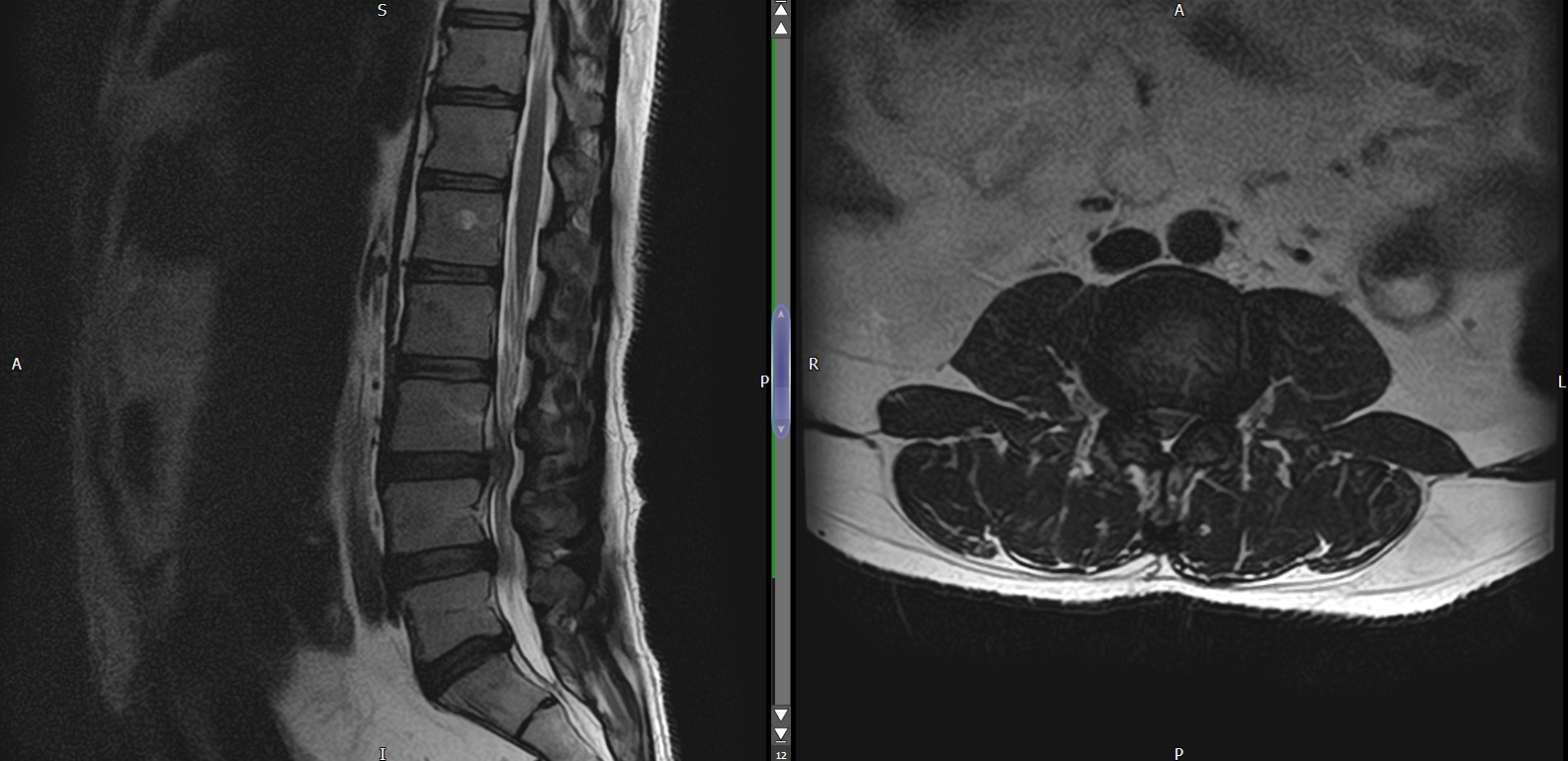
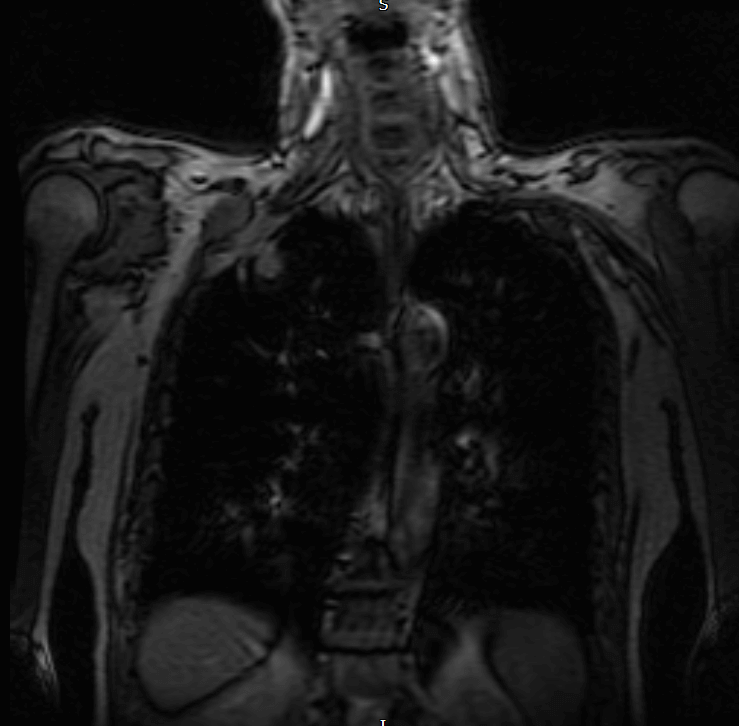
Worsening thoracic pain. Clinician orders MRI thoracic spine (urgent) to rule out any sinister pathology.
MRI Thoracic Spine reported as normal (11 days later).
MRI Thoracic Report
No signs of any bony suspicious lesions. No significant disc pathology.
No signs of cord compression
Clinician asks for clinic review.
★ Although the MRI thoracic is reported normal but the Localiser view is suspicious.
2nd Review – 2 weeks later
- 4 Month history
- (R) mid thoracic region pain around T5 – over the medial scapular area / rib cage.
- Pain wakes him up during the night time.
- Reports slight weight loss (on questioning) but doesn’t know how much.
- Tender over the (R) paraspinal T5 region. Palpable muscle which is more prominent on the right side when compared to the left.
- This seems like muscle tenderness but could also be bony tenderness in the rib cage.
Red Flags ⚑
- Thoracic pain
- Night pain
- Slight weight loss (patient not aware how much)
PLAN:
Clinician writes back to GP for –
- Repeat blood tests
- Request Chest X-ray
Results
- ESR: 28
- CRP: 5.6
- Chest X-ray
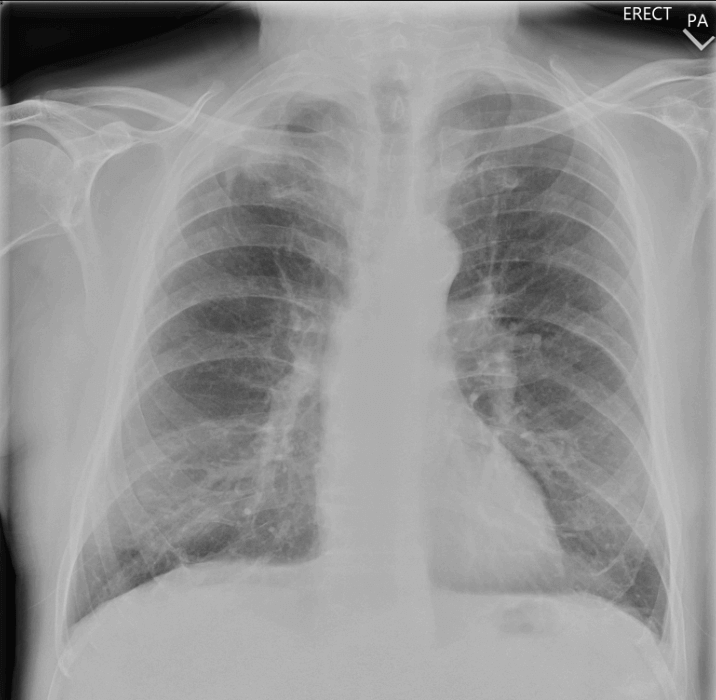
There is an ill-defined mass in the right apex measuring 2.7 cm. Urgent CT is required to evaluate this further.
CT Chest
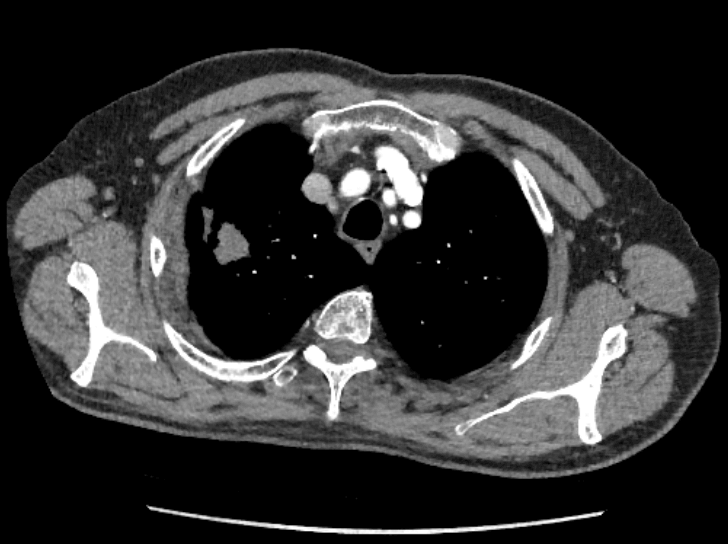
The current CT scan confirms the suspicion of a right apical mass. There is a 2.6 cm axial diameter spiculated mass in the apical segment of the right upper lobe which appears to also involve the pleural surface. There are background bilateral centrilobular emphysematous changes. There is a 6 mm right basal subpleural pulmonary nodule (series 4, image 246), probably an incidental intrapulmonary lymph node. No other significant focal pulmonary parenchymal abnormality or pleural effusion.
There is a right hilar node with a short axis diameter of 1.6 cm. There is no other significant supraclavicular, axillary, hilar or mediastinal lymphadenopathy.
Below the diaphragm, normal appearances of the liver and adrenals. There is no size significant upper abdominal/retroperitoneal lymphadenopathy.
No destructive bony lesion is seen.
Conclusions:
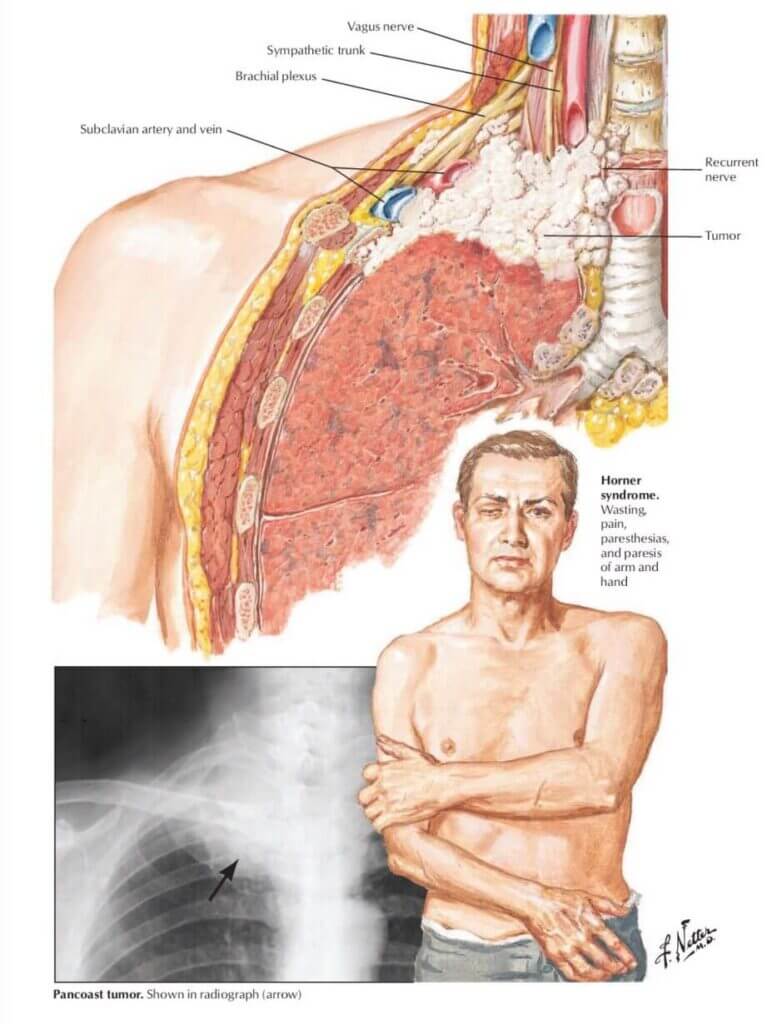
Likely right apical primary bronchogenic Pancoast tumour as described.
Medical history
- smokes cigarettes – 15/day
- Light drinker – 1-2 units per day
- BMI 25 kg/m2
- hypertension – on tablets
Learning Points
- History of smoking is worth asking in someone with chest pain / thoracic pain.
- Localiser views of the MRI can by helpful to view.
Calgary Guide Flowchart – Pancoast Tumour
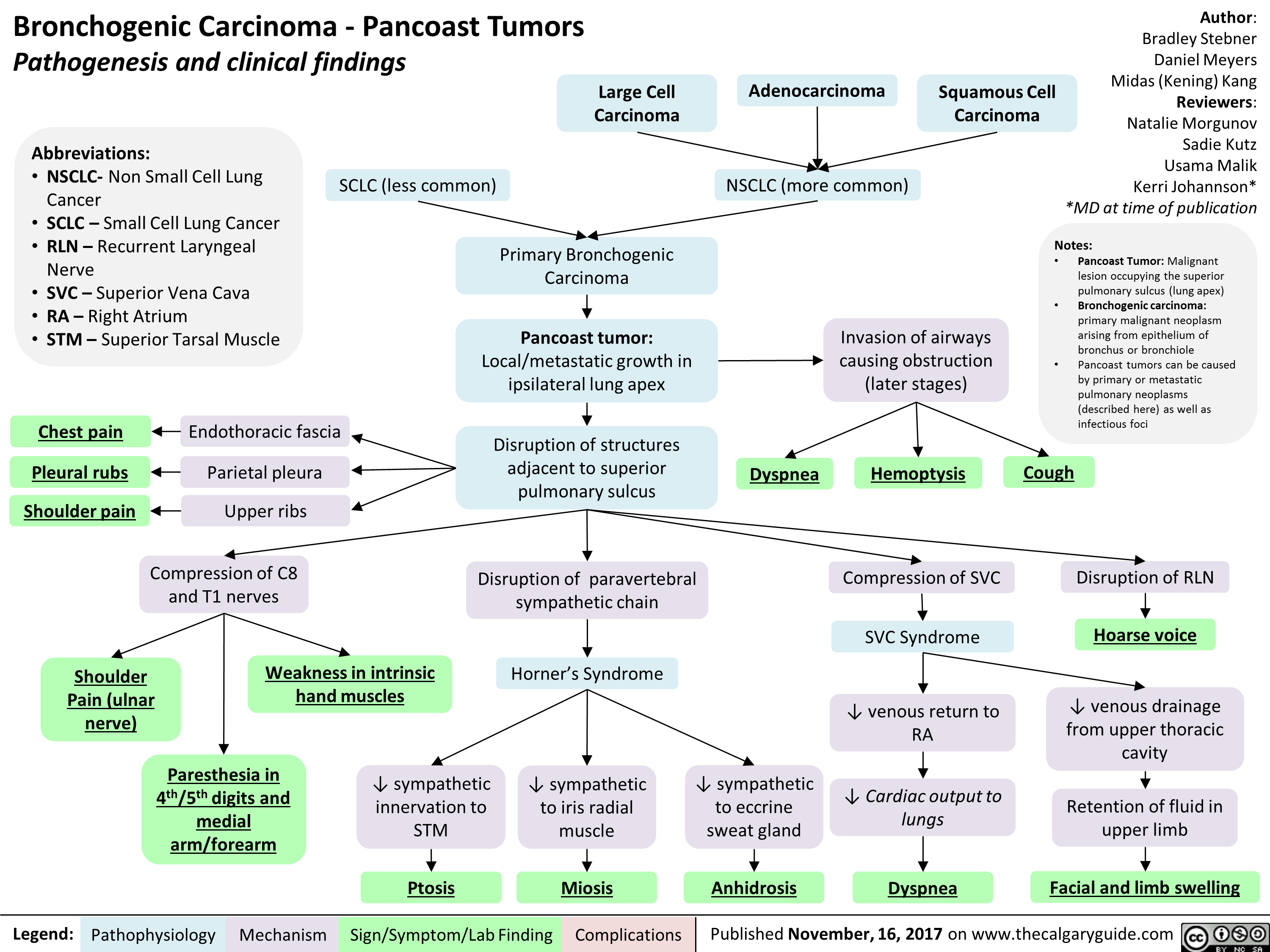
Pancoast Tumour – Associated Signs – Horners Syndrome
Ptosis – drooping eyelid. This happens when there is sympathetic disruption to superior tarsal muscle of the eyelid. This also elevates the eyelid. Levator palpebrae superioris is the other eye lid elevator.
Miosis – decreased pupil size. This happens due to sympathetic disruption to iris radial muscle.
Anhidrosis – decreased sweating on the affected side of your face due to sympathetic disruption to sweat glands.