Psoriatic Arthropathy
Published on May 11, 2022
Female 36
GP letter (March 2015) - presented to GP with 10 week history of painful swelling on right hand, just proximal to MCP joint of index finger on the dorsal aspect. Able to make a full fist. No history of injury. On examination soft tender swelling just lateral to right index finger MCP joint which becomes more prominent when fist is clenched. X-ray unremarkable.
GP letter doesn't mention any significant medical history.
MSK Department
Seen by ESP (March 2015) - findings - (R) Index finger MCP swollen, tender on palpation. No other joint is involved. Metacarpal squeeze is pain free. Patient reported that the finger is stiff in mornings.
Medical History - NAD
Impression - ? (R) Index finger MCPJ Synovitis.
ESP wrote back to GP requesting inflammatory markers along with uric acid. ESP also requested a US scan.
April 2015 - US scan showed thickening of extensor sheath with increased vascularity suggesting focal tenosynovitis.
May 2015 - Patient undergoes a US guided (R) index finger extensor tendon corticosteroid injection. Patient is then discharged back to GP.
****** Episode closed *****
GP Surgery
March 2016 - patient presents to GP with pain in 2nd MCP joint of (L) hand. Gives 2-3 week history for symptoms. GP requests x-ray hand.
April 2016 - GP refers to secondary care and queries whether this could be inflammatory arthritis as the patient has similar pain in the right hand 1 year ago. Referral is triaged to MSK department.
MSK
May 2016 - patient is seen in MSK by an orthopaedics doctor. Patient reports that she had similar symptoms in her (R) hand one year ago for which she had an injection and the pain settled. Keen on having the left hand injected too. Patient is referred for a US guided injection.
Aug 2016 - Patient gets her (L) index finger PIP joint injected under US guidance.
GP Surgery
July 2016 - Patient presents to GP complaining of foot pain. Reports that it has been present since March 2016 but has got much worse in the last 2-3 weeks. On examination the patient had tender MTP joints 4th > 3rd > 2nd toe.
- GP requests CRP, ESR, Rheumatoid Screen, Complement C3 and C4 and X-ray foot.
- Gets results of bloods the same day.
- CRP - 9, ESR - 2.
- NAD on Rheumatoid Screen and Complement. Rules out inflammatory pathology.
- Now awaits X-ray results.
Aug 2016 - X-ray is reported as unremarkable. Patient is referred to Podiatry. Patient meanwhile reports an improvement of symptoms with rest.
Oct 2016 - Patient consults GP again. GP notes the following -
- Patient has had (R) 2nd MCP joint injected followed by (L) 2nd PIP joint a year later.
- Has ongoing foot pain from MTP joints.
- Notices that 2 new joints have been involved - 3rd PIP on (R) and 3rd MCP on (L).
- Joints have boggy swelling and are tender.
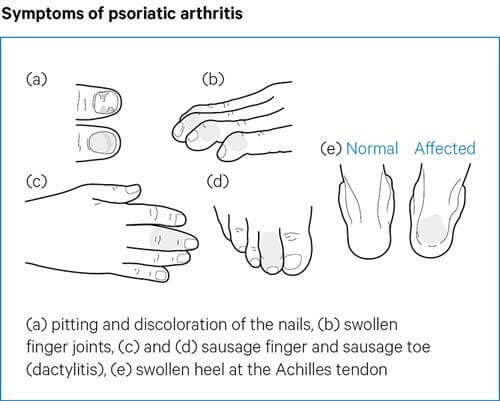
GP notices that patient has scalp Psoriasis, is presenting with Polyarthropathy. Suspects seronegative arthropathy with suspicion of Psoriatic Arthritis and refers urgently to Rheumatology.
Rheumatology
Nov 2016 - Patient is seen in Rheumatology and is diagnosed with Psoriatic Arthritis. Patient is started on Methotrexate. Later on is given intramuscular depomedrone, prescribed metoject, naproxen and Leflunomide (in various stages)
July 2017 - patient reports pain over (R) achilles. Enthesitis (R) Achilles is diagnosed.
Nov 2017 - achilles pain is ongoing. Rheumatologist request US scan.
Jan 2018 - patient undergoes US Guided injection of achilles tendon sheath.
March 2018 - patient is started on anti TNF - etanercept.
June 2018 - no help from etanercept. As her LFTs were deranged, DMARDs are stopped. Skin Psoriasis reappeared. Advised to start metoject.
Oct 2018 - Patient is started on Secukinumab.
Through 2019 - 2021, patient continues to have active synovitis despite being on biologics, NSAIDs, metoject and courses of prednisolone.
June 2021 - patient is started on Imraldi (Adalimumab).