Foot Pain
Published on Apr 14, 2022
78 Female
Apr 2017 - an object fell on to the left foot. No pain at the time. Pain in the foot started 3-4 months later.
Mar 2018 - GP requested x-ray (L) foot. NAD.
Apr 2019 - seen in physiotherapy. Patient reported that pain started after something fell on her left foot. Full ROM. Tender over cuniform, cuboid and navicular. Able to stand on toes. Gait slightly antalgic. Given exercises. Patient reported improvement.
Oct 2019 - fall in supermarket. Slipped and fell on floor, twisted both legs. Attended A&E. X-ray both feet and ankle - NAD.
April 2021 - presented to FCP in GP surgery. Reported pain in (L) foot. FCP documented previous history of falls. Very sensitive big toe and 2nd toe on palpation. FCP suspected midfoot OA and requested x-ray (L) foot. Referred to MSK for consideration of CSI if indicated.
May 2021 - seen in MSK. Patient reported the pain started after a fall. Had difficulty with weight bearing. Allodynia in whole of (L) mid and forefoot. No further assessment possible due to pain and patient being tearful. Dorsalis pedis and posteior tibial pulses absent.
- Medical History - COPD, stroke, cancer - non hodgkins lymphoma
Impression: ? Vascular, ? neuropathic
Clinician request MRI foot.
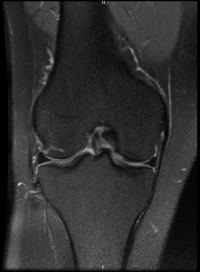
June 2021 - MRI foot - NAD
Normal alignment of the foot joints.
No stress or insufficiency fracture.
Osteoarthritis of the first metatarsophalangeal joint and medial tarsometatarsal junction is noted with minimal subchondral marrow oedema.
The sesamoids and plantar fat pad are well preserved.
No intermetatarsal bursitis or neuroma.
The distal flexor, extensor, peroneal tendons, plantar fascia and plantar plates are preserved.
Conclusion:Mild age-related degenerative changes. No clear source of severe forefoot pain.
June 2021 - Patient is referred back to GP for referral on for vascular review
Aug 2021 - patient is referred to Vascular Surgery
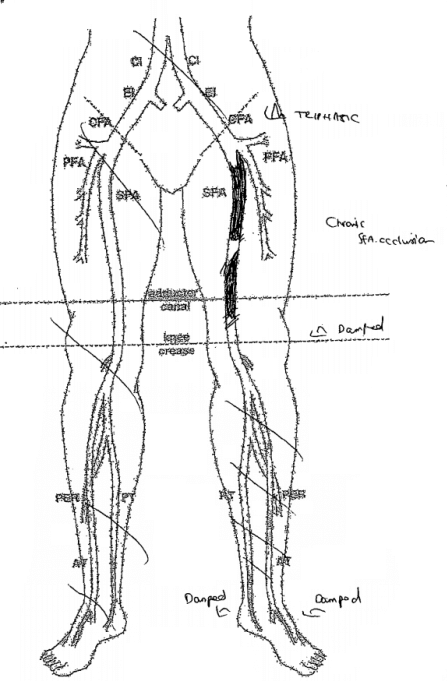
Oct 2021 - seen in Vascular surgery. Notes - (L) good femoral, nil palpable below. Right full compliment of palpable pulses.
Duplex scan left - Triphasic signal CFA, Chronic occlusion of SFA damped signal at foot.
US Doppler lower limb arteries Lt
- The CFA and proximal ProfA are patent with triphasic flows.
- The prox-mid SFA is occluded.
- The PopA is patent with monophasic flow.
- Poor assessment of the crurals due to low flows.
- The PTA and ATA are patent distally with damped flows.
Offered SFA Angioplasty.
Vascular Notes
Conclusion
- History of trauma (fall) caused most confusion.
- Checking pulses should be routine part of foot exam.
- MRI was done to rule out any sinister pathology (due to history of lymphoma) and also to check for any inflammatory / occult pathology.
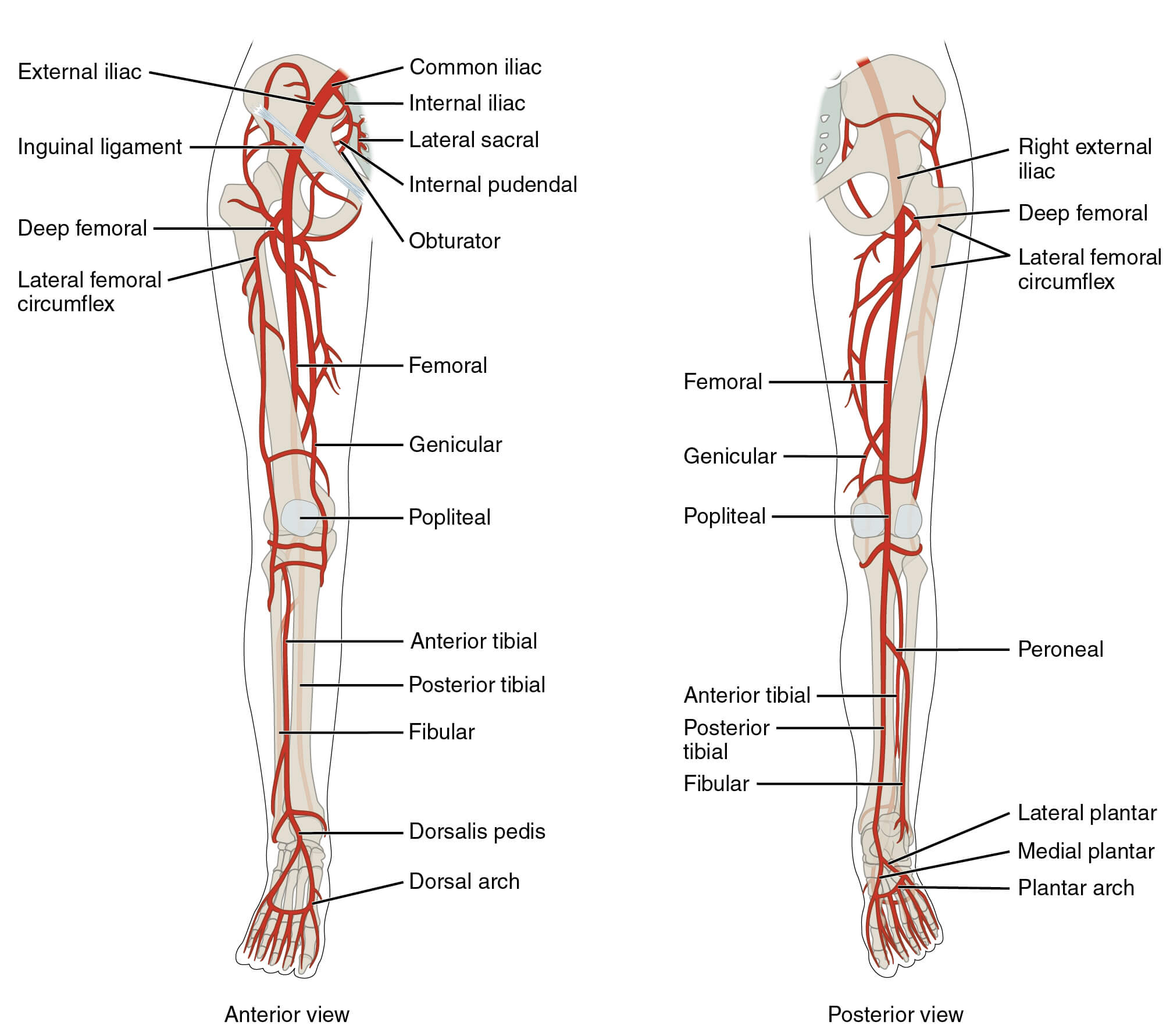
Lower Limb Arterial Supply