Summarised from Rx of Pseudogout
Pseudogout - acute attack of synovitis induced by calcium pyrophosphate dihydrate (CPPD) crystals.
- It has presentation similar to gout and inflammatory arthritis
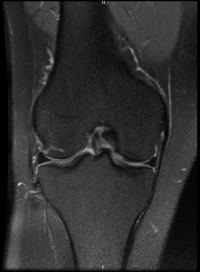
- Knee is the most commonly involved joint, followed by the wrist, ankle, elbow, toe, shoulder and hip.
- Presentation can be spontaneous or provoked by trauma.
- Flares of pseudogout after parathyroidectomy are well described.
- Pamidronate therapy for hypercalcaemia has also been implicated as a trigger for acute attacks of pseudogout.
- Pseudogout is confirmed by the demonstration of CPPD crystals in synovial fluid which manifest as rhomboid-shaped rod-like structures that exhibit weakly positive or no birefringence by compensated polarized light microscopy, in contrast to the negatively birefringent needle-shaped MSU crystals found in gout.
- Gout and pseudogout may also coexist in a single inflammatory effusion, as 20% of patients with CPPD will have hyperuricaemia and a quarter of these will develop gout at some stage.
Asymptomatic Chondrocalcinosis
- Chondrocalcinosis refers to calcification seen in cartilage on radiographs.
- It is commonly present in patients with CPPD deposition disease, but is neither sensitive nor specific for affected patients.
Pseudo RA
- A small proportion (<5%) of patients with CPPD deposition experience a nonerosive, asynchronous, inflammatory arthritis which mimics RA .
- The associated morning stiffness, malaise, synovial thickening, symmetrical involvement, flexion contractures and elevated acute phase inflammatory markers often lead to a misdiagnosis of RA.
- In addition, 10% of these individuals, who are often of older age, will have low titres of rheumatoid factor thus causing further diagnostic confusion.
- Therefore, the presence of CPPD crystals in synovial fluid and radiographic changes more in keeping with OA favour a diagnosis of pseudo-RA, while elevated titres of anticyclic citrullinated peptide (anti-CCP) antibodies and the presence of bony erosions either on ultrasound or plain film radiographic imaging indicate a diagnosis of classical RA.