Causes
- Trauma – incision (broken glass), fracture, dislocation, gun shot wound, stab wound.
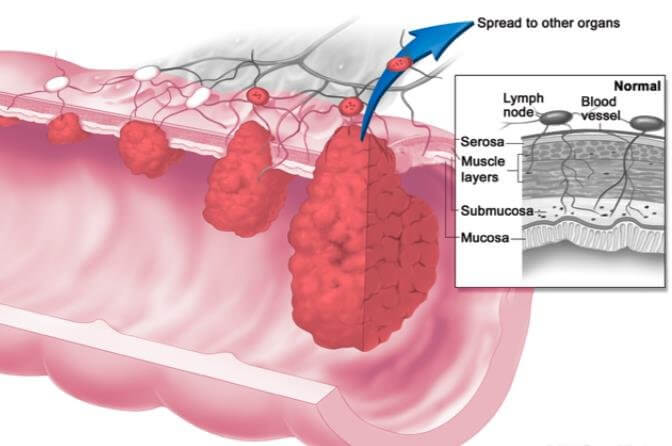
- Infiltration of nerve by a malignant growth
- Sometimes, the nerve lesion happens spontaneously. Worth asking in such cases, if they have had any injections near the site of a nerve. Or if they are a diabetic, alcoholic or work with lead or arsenic.
- Patients with Diabetes or leprosy may have loss of sensation in a patch of a skin.
Associations
- Fracture shaft of humerus – associated with radial nerve injury.
- Supracondylar fracture of elbow – median, ulnar or radial nerve may be injured.
- Medial epicondyle fracture – associated with ulnar nerve injury.
In both the supracondylar fracture and the fracture of the medial epicondyle, there may be late paralysis of the ulnar nerve which is known as ‘tardy ulnar palsy‘ — due to involvement of the nerve in callus formation.
- Fracture neck of fibula – lateral popliteal nerve may be injured.
- Subcoracoid dislocation of the humerus and fracture of the neck of the humerus – axillary nerve may be injured leading to paralysis of the deltoid.
- Posterior dislocation of the hip, subtrochanteric fracture and supra-condylar fracture of the femur – sciatic nerve may be injured. Generally common peroneal portion of sciatic nerve is injured.
Examination
Inspection
- Wrist Drop – Radial nerve
- Foot Drop – lateral popliteal nerve
- Winging of Scapula – serratus anterior, long thoracic nerve
- Ulnar claw hand (Main en Griffe) – Ulnar nerve
- Ape thumb – median nerve, opponens pollicis
- Pointing index – median nerve, lateral half of flexor digitorum profundus
Wasting
- Deltoid
- Thenar eminence
- Hypothenar eminence
- Hollows between the metacarpals – due to atrophy of the interossei
Nerve / Muscle Testing
- Accessory Nerve – Trapezius – Check resisted shoulder shrug.
- Hypoglossal Nerve – Tongue – Patient is asked to protrude the tongue. Tip of tongue will deviate towards the side of the lesion (in case of hypoglossal nerve involvement).
- Long Thoracic Nerve – Serratus Anterior – Winging of scapula on resisted scapular protraction.
- Axillary Nerve – Deltoid – Resist shoulder abduction. Also palpate the deltoid to check muscle contraction.
Radial Nerve
- Brachioradialis – resist midprone elbow flexion. Brachioradialis will stand out.
- Wrist Joint Extensor Muscles – apart from Extensor Carpi Radialis Longus, all other wrist extensors are innervated by Posterior Interosseous nerve. Paralysis of these muscles causes a wrist drop. Check resisted wrist extension for weakness.
- Extensor Digitorum – causes extension at MCP joints. It also extends the interphalangeal joints along with the corresponding interossei and lumbricals.
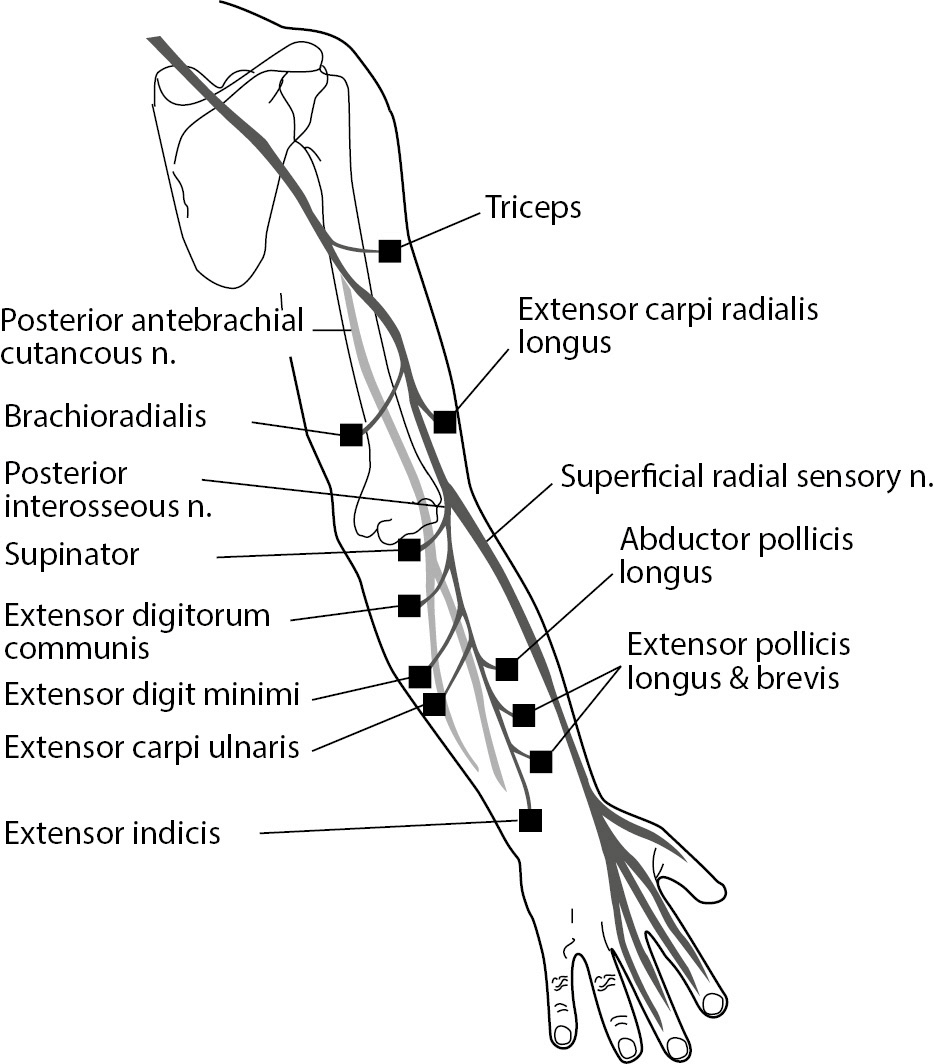
- So when this muscle is paralysed the patient will not be able to extend the MCP joints but will be able to extend the IP joints to some extent.
Median Nerve
- Flexor Pollicis Longus – Stabilise the proximal phalanx and then resist thumb IP flexion. This muscle is only paralysed when the median nerve is injured at or above the elbow.
- Flexor Digitorum Superficialis & Profundus (lateral half) – Ask patient to clasp the hands. The index finger remains pointing (doesn’t flex). This is called “Pointing Index“. Test is also called Ochsner’s clasping test.
- Abductor Pollicis Brevis – This muscle is concerned in abduction of the thumb that means the thumb moves upwards at right angle to the palm of the hand when the hand is laid flat on the table. This is done by asking the patient to touch the pen which is kept at a slight higher level than the palm of the hand with the thumb. This is known as pen test.
- Opponens Pollicis – This muscle swings the thumb across the palm to touch the tips of the other fingers. The patient with paralysis of this muscle will be unable to do this movement. The students must not forget that a vicarious movement short of proper opposition movement is possible by adductor pollicis supplied by the ulnar nerve.
Ulnar Nerve
Flexor Carpi Ulnaris
Interossei
First palmar interosseous and adductor pollicis