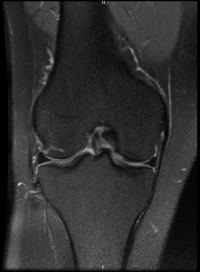
Knee OA
- 40% of patients over 70 years old have symptomatic knee osteoarthritis.
- Prevalence higher in females.
- Up to 50% of patients with radiographic knee osteoarthritis do not experience regular pain.
Osteoarthritis is a disease of the Whole Joint - apart from cartilage it also affects other structures. Other features are
- Inflamed synovium
- reduced viscosity of synovial fluid
- Thickened subchondral bone
- Thickened capsule
- Cruciate ligament destruction
Ref - Thijssen et al 2015 - Recommendations
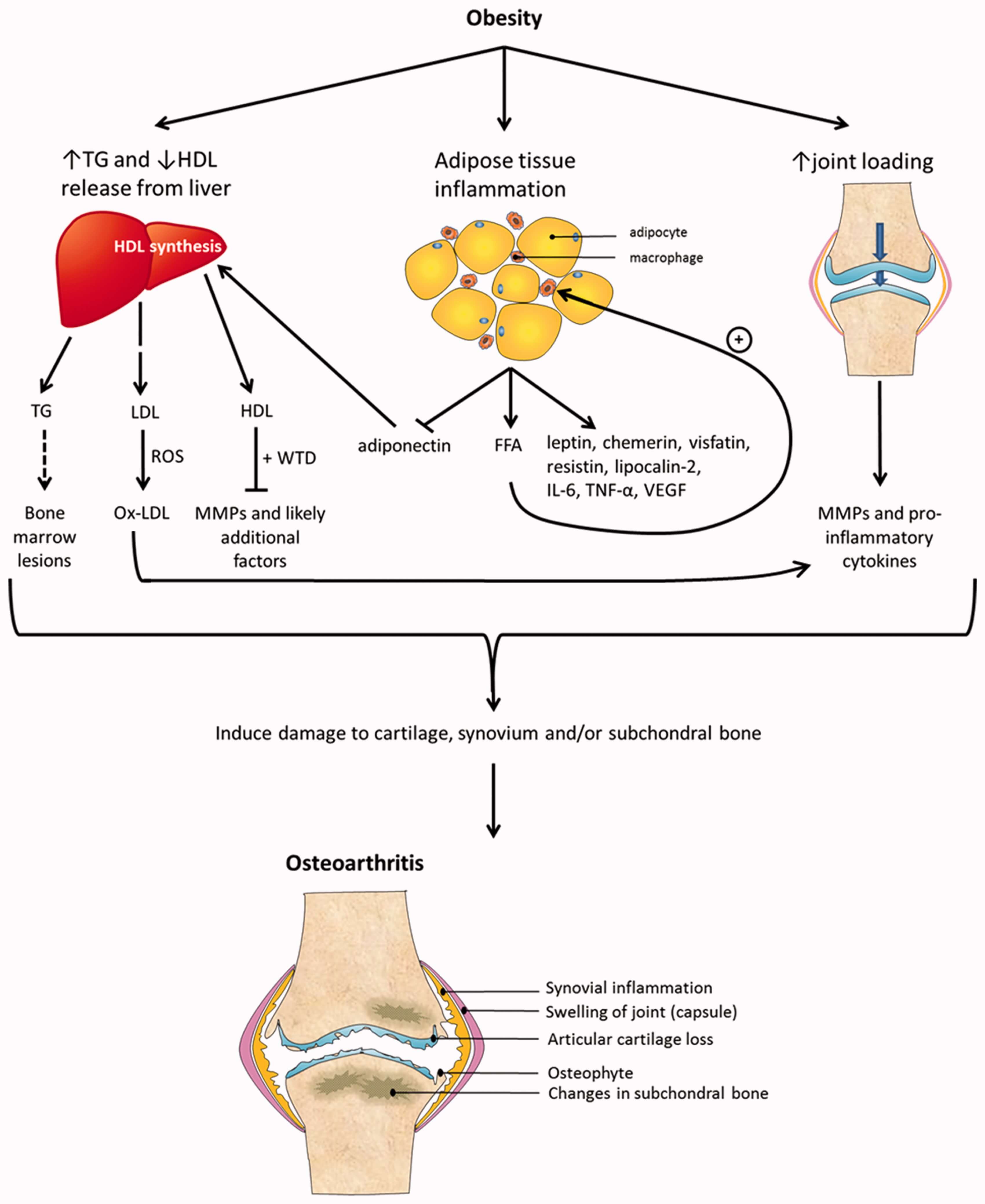
- The link between obesity and OA transcends excessive loading.
- Inflamed adipose tissue and obesity-related dyslipidaemia play pivotal roles in obesity-induced OA.
- Targeting adipokines and cytokines might benefit obese OA patients.
Obesity and OA
- It is established that obesity is a risk factor for developing OA.
- Central obesity is a particularly associated with OA. Apart from load bearing joints, people with central adiposity also get hand OA. It is thought it is related to cytokines secreted by adipose tissue.
- Adipose tissue is an endocrine tissue, which secretes cytokines (adipokines)
Valgus needs surgery earlier than varus as it is technically difficult with valgus and leads to less better outcomes.
NICE OA (2014)
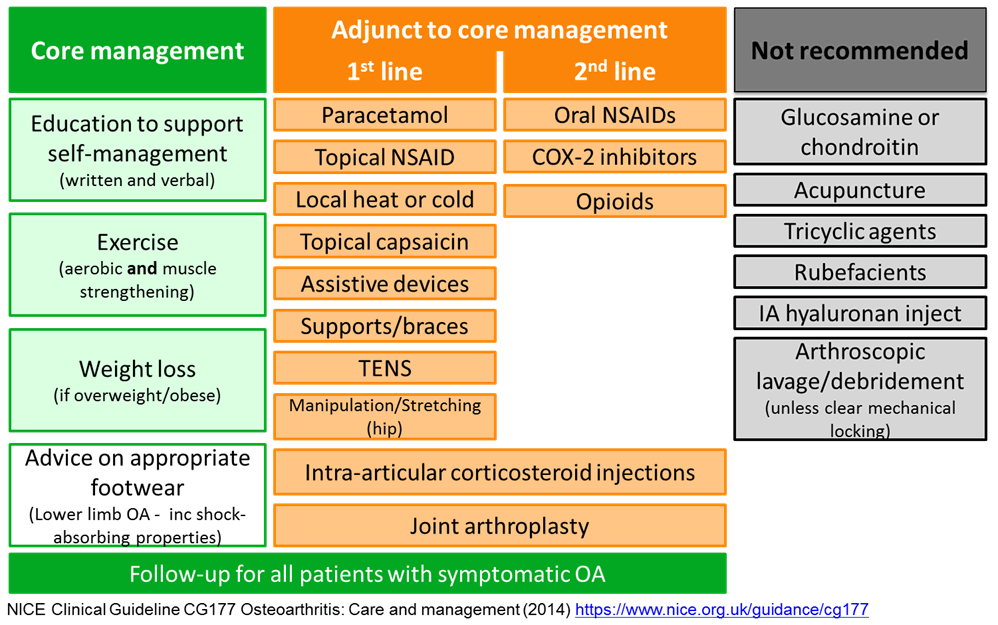
Education
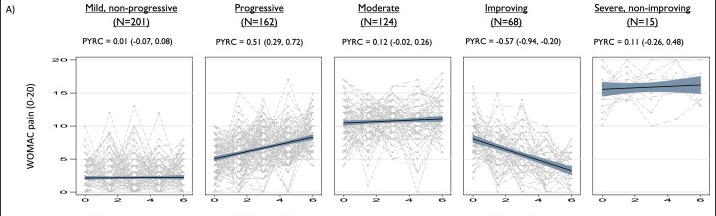
Progression of OA
Nicholls et atl 2014 - Conclusion
Our findings strengthen the grounds for moving beyond a simple stereotype of osteoarthritis as “slowly progressive”. Mild, non-progressive or improving symptom trajectories, although difficult to reproduce, can nevertheless represent a genuinely favourable prognosis for a sizeable minority.
Exercise
Bennell et al 2015
- Strategies for weight loss and exercise, as well as the use of appliances for biomechanical modification, should be tailored to the individual patient, rather than using a 'one size fits all' approach.
- A patient suffering from varus thrust during walking (which is related to joint instability and lack of confidence in the knee) is likely to benefit from neuromuscular exercise,
- Whereas an obese patient with muscle weakness is likely to benefit from strength training.
Personalised exercise programme is better at addressing OA.
Exercises must be continued. Benefits are lost after 6 months of stopping exercise.
Thomas et al 2022
The current study found high-quality evidence to support the use of hip abductor muscle strengthening exercises as a rehabilitative treatment for subjects with knee osteoarthritis.
Is exercise safe for patients with OA?
Quicke et al 2015
There was no evidence of serious adverse events, increases in pain, decreases in physical function, progression of structural OA on imaging or increased TKR at group level. The case control study concluded that increasing levels of regular physical activity was associated with lower risk of progression to TKR.
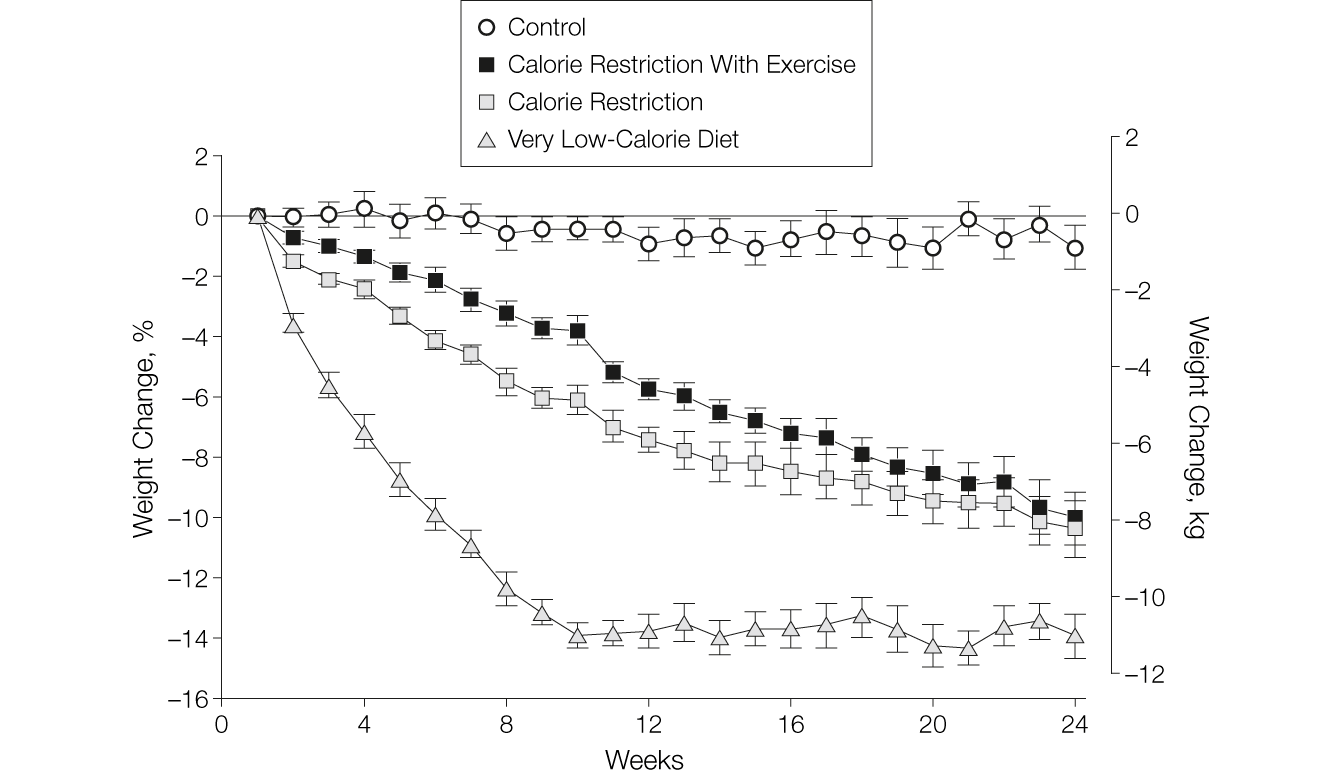
Weight Loss
Calorie restriction works well for weight loss - Heilbronn et al
Intra-articular Steroid Injections
McAlindon et al 2017
- Intra-articular triamcinolone compared with intra-articular saline.
- At 2 years significantly greater cartilage volume loss and no significant difference in knee pain.
John Orchard 2020 - BMJ
- Intra-articular corticosteroid injections possibly improve pain and function in the short term (<8 weeks) in patients with osteoarthritis of the knee, but the evidence is of low quality, and any benefit is not usually sustained beyond 3 months.
- Emerging evidence suggests a possible small risk of joint deterioration and worsening symptoms over the long term with intraarticular corticosteroid injections.
- Consider the severity of pain, feasibility of other treatment options including exercise, and the patient’s preferences regarding risks and benefits when planning treatment.
Wijn et al 2020
Corticosteroid injections seem to be associated with an increased risk of knee arthroplasty in patients with, or at risk of developing, symptomatic OA of the knee. These findings suggest that a conservative approach regarding the treatment of these patients with corticosteroid injections should be recommended
Ref:
Obesity and osteoarthritis, more than just wear and tear: pivotal roles for inflamed adipose tissue and dyslipidaemia in obesity-induced osteoarthritis - Thijssen et al, Rheumatology, Volume 54, Issue 4, April 2015
Pain trajectory groups in persons with, or at high risk of, knee osteoarthritis: findings from the Knee Clinical Assessment Study and the Osteoarthritis Initiative - E. Nicholls et al. / Osteoarthritis and Cartilage 22 (2014)
Influence of biomechanical characteristics on pain and function outcome from exercise - Bennell et at 2015
Is long-term physical activity safe for older adults with knee pain?: a systematic review - Quicke et al 2015
Effect of 6-Month Calorie Restriction on Biomarkers of Longevity, Metabolic Adaptation, and Oxidative Stress in Overweight Individuals - Heilbronn et al 2006
Effect of Intra-articular Triamcinolone vs Saline on Knee Cartilage Volume and Pain in Patients With Knee Osteoarthritis - McAlindon 2017
Is there a place for intra-articular corticosteroid injections in the treatment of knee osteoarthritis? - John Orchard 2020 BMJ
Intra-articular corticosteroid injections increase the risk of requiring knee arthroplasty - Wijn et al 2020
Hip abductor strengthening in patients diagnosed with knee osteoarthritis – a systematic review and meta-analysis - Thomas et al 2022